



1. Introduction
Quality management is an important issue in health care industry. In the beginning the theory ‘quality’ focused on production. By the time the concept developed to service and process. Nowadays, the quality expanded to social orientation (Al-Ibrahim 2014, 123-147). Health care market is also changing from producer oriented to customer oriented. It is due to increasing customer’s impact and public pressures. Consequently, the patient is a customer in health care organizations, or the person who participates in decision making process (Balasubramanian 2016, 271-278). From this point, it is important to know who would be the major customer in healthcare industry. And their decision making empowerment.
Numerous researchers and nonprofit organizations have taken efforts to analyze women empowerment. Women empowerment has a significant value for the development of a society. It improves the quantity and the quality of human resources. In result it can play an important role in changing society positively (Gupta and Yesudian 2006, 365-380). Women empowerment is a multidimensional concept that may defined from various perspectives (Hameed et al. 2014). However, we have to mention that there exists context dependency for women empowerment measures. It may be used based on familial and social context (Pratley 2016, 119-131). United Nations Statistics Division (UNSD) defines it as women and girls getting power and control over their own lives. Other authors defined as mastery and participation, social good and goal achievement (Cattaneo and Chapman 2010, 646).
Ethiopia is an ancient country with diverse nationality and cultures. According to World Health Organization (WHO) the health policy was initiated for the first time in 1960 in Ethiopia (EDHS 2005). Some studies found that maternal health care service utilization is very low and below acceptable standards in Ethiopia (Tarekegn, Lieberman, and Giedraitis 2014, 161; Tiruneh, Chuang, and Chuang 2017, 718). Hence many organizations have taken an effort to improve the women empowerment in Ethiopia. “Leave No Woman Behind” is the Joint Programme aimed to empower women in Ethiopia (UNWOMEN 2016). In Ethiopia economic and socio-political and cultural agendas remains as challenge concerning to women’s decision making participation among women. 303,000 women worldwide died during the pregnancy, after childbirth, which most of those deaths were from sub-Saharan Africa (WHO and Mathers 2017). Additionally, (WHO 2018) reported that women face difficulties due to female genital mutilation (FGM). FGM is mostly practiced on young girls. 23.8 million Ethiopian women and girls had undergone FGM (UNICEF 2013). World Health Assembly emphasized the need for concerted action in all following sectors: education, health, finance, justice and women’s empowerment on the elimination of FGM (WHO 2018). According DHS 2011 report almost a quarter of Ethiopian women do not decide on most individual and household issues. Birth control methods and seeking for the assistance of trained provider are more likely made by their husbands. Furthermore, women in Ethiopia suffer from harmful traditional practices, early marriage and childbearing (USAID 2018).
Health care industry needs to consider the potential costumers among women like in Ethiopia, who may make decisions on their own healthcare in future. The product or service which were prepared in upstream stage might not be always effective. Hence, it is very meaningful to figure out the factors which influence to the new market. From this point, the impact of decision making of women empowerment has a significant implication from the holistic perspective. Even though now patriarchal decision making domains in households, we have to consider about the new market. Grasping a market is a critical issue. In order to figure out the potential customers in health care industry, the social quality issue must be analyzed in downstream stage. Consequently, the society may change from male dominate customer to women customer market. If by years the market will change, we may see possibility of creating the new market.
The purpose of this study is to explore the health care decision making of Ethiopian women at household level. In order to give more practical suggestions, we will use Ethiopia Demographic Health Survey (EDHS) 2005 & 2016, which provided data about currently married women. Moreover, our aim is to understand the factors that influence to potential customers in healthcare industry in social quality level. There are many advantages of discovering potential costumers in healthcare industry in society. It will give a chance to healthcare management industry to create a new market and to improve the social quality level. In parallel, it will help to Ethiopian women to get a high level of service quality in healthcare industry.
The main goals are as following: 1) Do the mobility of decision making impacts the health care decision making of women? 2) Do the mobility and health care decision making’s vary in degree according the influence of economic decision making? 3) Are there any changes of women’s empowerment in Ethiopia between two periods 2005 and 2016?
2. Literature review
2.1 Women empowerment
Women empowerment is very complex and multidimensional concept. There are three inter-related dimensions of women’s empowerment: resources are describes as access, material and human, social resources; agency is the process of decision making; finally achievement is well-being outcomes (Kabeer 1999, 435-464). Social quality management have to pay attention on potential customers in health care industry. Other researchers explained the concept of women’s empowerment in six dimensions and in the household, community, and broader arenas levels. There are economic, socio-cultural, familial/interpersonal, legal, political, psychological dimensions. Based on these dimensions the upper mentioned concept might be defined in different dimensions and levels (Phan 2016, 359-378; Mahmud, Shah, and Becker 2012, 610-619). This is why it is challenging to gather enough data on women’s empowerment in all levels to measure process (Phan 2016, 359-378; Woldemicael 2010, 599-620).
2.2 Women empowerment in decision making
Since 1999-2000 Demographic Health Surveys (DHS) implemented additional information concerning to women’s empowerment indicators. The women’s participation in household decisions is one of the main indicators in DHS. Studies analyzed women’s empowerment in the domestic perspective: economic decision making power on major purchases, physical freedom in visiting some local facilities, etc.. (Mason and Smith 2003). Participating in making several decisions regarding their own health care, larger household purchases, visits to family and friends impacts to women’s empowerment (Pratley and Sandberg , 1-17). Economic empowerment of women help them to improve their health and well-being (Roy and Chaudhuri 2008, 1951-1962). Women autonomy on health care decision plays an important role for their maternal and child health outcomes (Acharya et al. 2010, 15).
Early studies focused the influence women’s empowerment to maternal health service utilization in Ethiopia. Socio-demographic factors, regarding women autonomy variables used women’s health care spending (Tarekegn, Lieberman, and Giedraitis 2014, 161). Some studies analyzed on community and individual levels of women autonomy (Tiruneh, Chuang, and Chuang 2017, 718). In this study, we focus on household level of women empowerment. Since one of the important domain in woman’s life is household, there is a meaningful implications in research (Phan 2016, 359-378).
3. Methodology
3.1 Data selection
For the current study the secondary data from the 2005 and 2016 Ethiopia Demographic and Health Survey panel (EDHS) were used. The survey data were downloaded from the Measure DHS website after permission. EDHS is a national representative survey of women age 15-49. It was funded by the United States Agency for International Development (USAID) and was implemented by the Ethiopian Central Statistical Agency. The main goal of EDHS is to provide the detailed information on fertility, family planning, infant, child, adult and maternal mortality, maternal and child health. EDHS conducted four times surveys (2000, 2005, 2011, 2016).
3.2 Sample selection.
This study used Ethiopian married women age 15-49. The variables were selected from the Women’s Questionnaire. For this study only two periods were chosen to test women’s empowerment in health care, economic, mobility decision makings in household level. The target are only married women, the sample of men were not used.
3.3 Procedure of data reduction.
It is important to mention that we used two periods of DHS data. Though the variables are identical, the sample size is different. Firstly, provided the data reduction and preparation for 2005 year. Initially, the sample size was 14,070 women. However, due to the study purpose implemented data reduction. The data reduction progressed by the following criteria. The first criteria was marital status of women. Since study focused only on married women, who are in union currently. It was necessary to recode the marital status, in order to select only married women. The marital status in questionnaire was coded as following: 0=never married, 1= married, 2= living together, 3=widowed, 4=divorced, 5=not living together. However, we selected only 1= married and 2=living together answers. Other answers excluded from the research. In result, the sample size reduced from 14,070 to 8,644. The reason why we selected only married women is connected with the second criteria of the data reduction. There three main variables: health care decision making, mobility and economic decision making of women. In secondary data the original name and codes were as following:
Question: Final say on own health care (health care decision making), final say on visits to family or relatives (mobility decision making), final say on making large household purchases (economic decision making). Response: 1=respondent alone, 2=respondent and husband/partner, 3=other person, 4=husband/partner alone, 5=someone else.
However, for the research the following response were recoded. We selected 1=respondent alone and 4=husband/partner alone and renamed respondent alone as ‘me’ who is woman (Woldemicael 2010, 599-620). The issue individual or joint decision’s measurement might be different by studies. On the other hand, according to other researchers woman is autonomous if she is able to decide alone or with her husband (Tarekegn, Lieberman, and Giedraitis 2014, 161).
Consequently, from the first reduced data sample 8,644 remained only 2003 sample size. The major reason of the rapid decrease data sample size due to the excluded answers. Additionally, the missing value was deleted, too. Secondly, the data reduction was provided for 2016 year sample size with the similar process as 2005 year. Generally, the initial sample size was 15,683 which was reduces to 2,317 final sample size. However, due to the first criteria the marital status was recoded. According to the second criteria three main variables: health care decision making, mobility and economic decision making of women are recoded as the first sample survey.
3.4 Research model
3.4.1 Research questions
1) Do the mobility of decision making impacts the health care decision making of women?
2) Do the mobility and health care decision making’s vary in degree according the influence of economic decision making?
3) Are there any changes of women’s empowerment in Ethiopia between two periods 2005 and 2016?
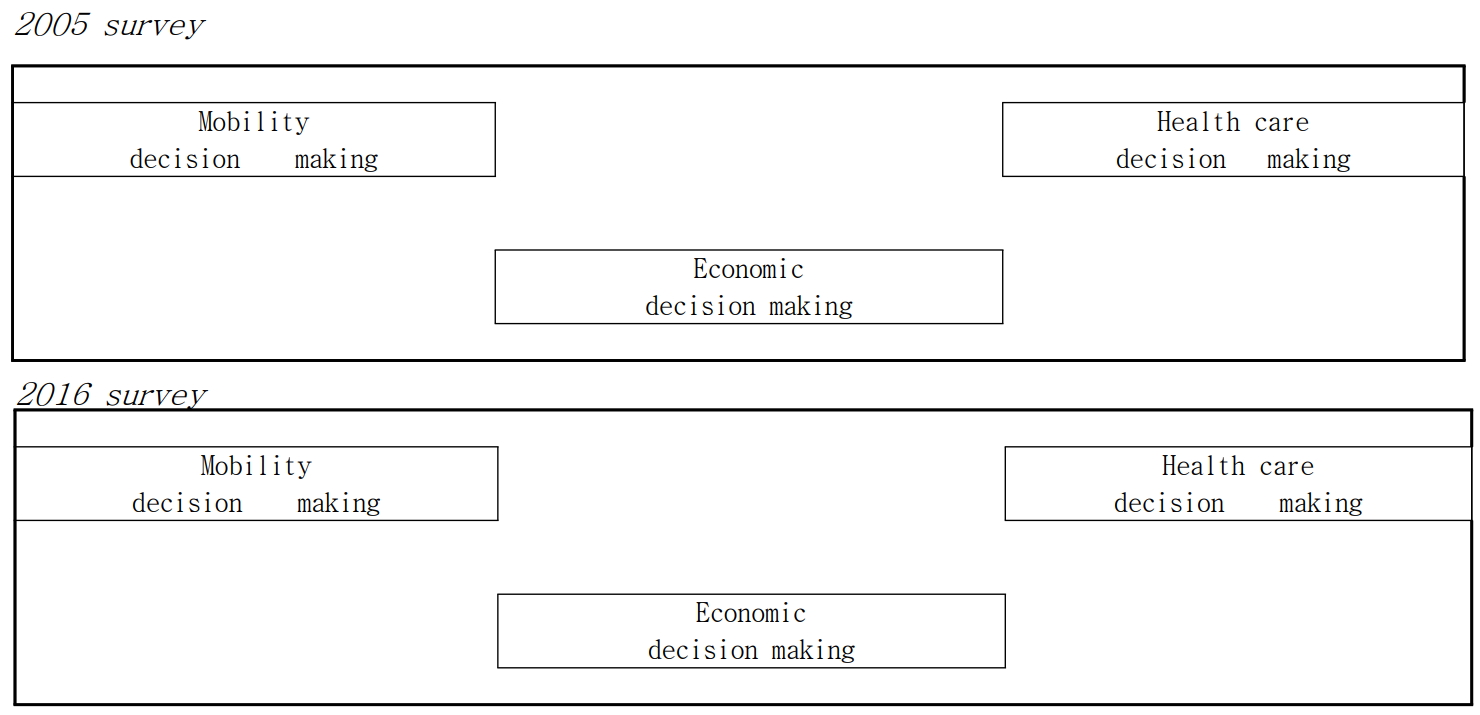
Conceptual framework: based on Andersen’s emerging model for assessing human behaviors with reference to utilization of health services (Andersen 1995, 1-10; Tulsi Ram 2015a)
3.5 Statistical analysis
Data analysis were performed in the following sequence: descriptive statistics, Pearson correlation, Chi-square test, and finally the logistic regression. Firstly, Pearson analysis were conducted to examine the relationship among all variables, which shows Pearson correlation coefficients. We selected only high correlated variables through Pearson Correlation. (Correlation coefficients 0.5<0.7). Chi-squared test were performed as well. Finally, the logistic regression analysis were conducted in three models. Logistic regression conducted with three representative variables (independent variable: mobility decision making, control variable: economic decision making, dependent variable: health care decision making). In the first model was run independent variable (mobility decision making) with control variable (economic decision making). In the second model was tested independent variable (mobility decision making) with dependent variable (health care decision making). In the last model we performed independent variable and control variable with dependent variable. The criteria for accepting the next model was to get a significant p value (0.0001***) and Normalized Beta Value of variables. The process continued until getting the final model.
4. Result
The study analyzed the women’s empowerment in making health care decisions by using two periods of DHS data. More specifically, we explored links between the mobility and economic decision makings to health care decision making of women. And analyzed the changings of women’s decision making empowerment between two survey periods. In result, the mobility decision making has an association with health care decision making of women. Moreover, economic decision making of women has an moderate effect.
4.1 The result of Pearson correlation
Pearson correlation was conducted for both period of surveys. The goal of this analysis was to measure of the strength of the association between variables. At first, all variables were conducted. However, except the three main variables there were not significance of correlation. Thus we conducted the second time for Pearson correlation with following variables: independent variable (mobility decision making), moderator variable (economic decision making), dependent variable (health care decision making). The tables 1 and 2 show the results of Pearson correlation of two surveys.
4.2 The result of socio demographic characteristics.
According descriptive analyses of women for both surveys showed as following: Women aged 15-49 are mostly like with low literacy and education. Furthermore, 79% of women are non employment and poor social media access for the first period of survey (2005). In the second survey (2016) even though it did not changed significantly, only literacy level improved by 10%.
Table 3.
Socio demographic characteristics
4.3 The results of Chi-square test
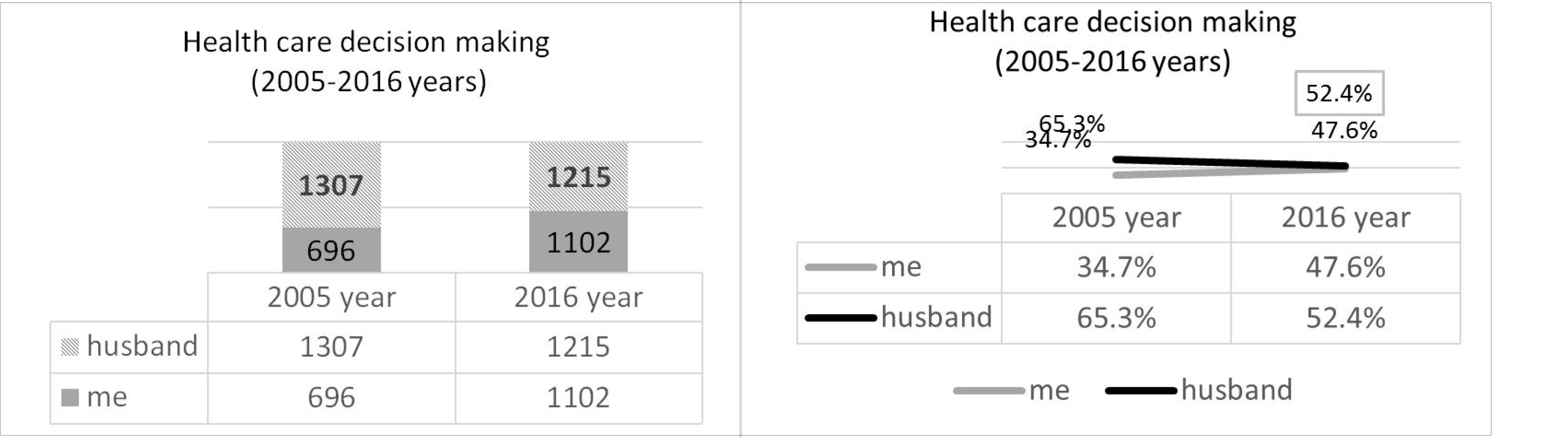
In this study we performed the chi-square test with the following variables as Pearson correlation. The tables 4 and 5 show the result of chi-square test of two surveys. As demonstrated in Table 4 and 5, chi-square analysis showed significant difference between respondents in both surveys. The chi-square test results of decision making of health care and mobility were significant statistically with a p-value 0.0001. Regarding to decision making on health care was found that 35 % of respondents in first survey decided for their own health care by themselves. While 65% of respondents’ decision making on their own health care was made by their husbands. On the other hand, in second survey 48% of women decided for their own health care by themselves, and 52% of women’s health care decision making was made by their husbands or partners.
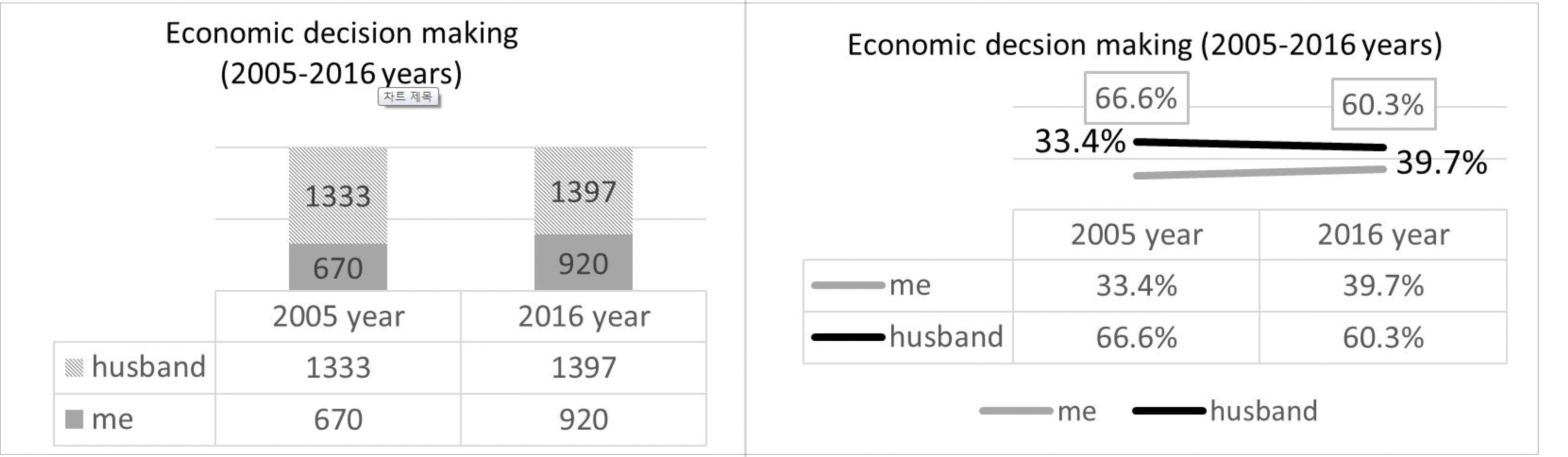
For the individual compared variables were demonstrated in the following graphs. In these figures were presented clearly how the decision making empowerment of women had changed by years.

4.4 The results of Logistic Regression analyses
According table 6 (2005 survey) results showed that the Normalized Beta Value of mobility decision making is 2.567 with p value 0.0001 in model 2, in comparison the Normalized Beta Value mobility decision making is 1.901 with p value 0.0001, for economic decision making is 2.1 with p value 0.0001 in model 3. Based on these results the Normalized Beta Value of independent variable mobility decision making is high in the model 2, however the Normalized Beta Value of mobility decision making decreased in model 3. Based on this result there is moderate effect.
According table 7 (2016 survey) the Normalized Beta Value of mobility decision making is 3.727 with p value 0.0001 in model 2, in comparison the Normalized Beta Value is 2.816 with p value 0.0001, for economic decision making is 2.796 with p value 0.0001 in model 3.
According to logistic regression analyses the Normalized Beta Value of health care decision making and mobility decision making for both years (2005 and 2016) decreased when the moderator economic decision making existed.
Table 6.
Health care decision making, mobility decision making, economic decision making (Logistic regression analyses of 2005 year)
Table 7.
Health care decision making, mobility decision making, economic decision making (Logistic regression analyses of 2016 year)
5. Conclusion
The purpose of this study is to analyze the health care decision making of Ethiopian women at household level. And to understand the factors that influence to potential costumers in healthcare industry in social quality level. The main goals are as following: 1) Do the mobility of decision making impacts the health care decision making of women? 2) Do the mobility and health care decision making’s vary in degree according the influence of economic decision making? 3) Are there any changes of women’s empowerment in Ethiopia between two periods 2005 and 2016?
The first major finding although is not significantly related to health decision making of women, statistically some clear relationship exist. The mobility decision making impacts the health care decision making of women. Based on results the Normalized Beta value of mobility decision making is high in model 2 for both surveys (Beta value 2.567 in model 2 vs 1.901 in model 3, Beta value 3.727 in model 2 vs 2.816 in model 3). The present study tried to explore the behavior regarding health care decision making through their mobility decision making. In result, we found that there is a positive relationship between mobility and health care decision making. Women are likely decide regarding to their own health care by themselves, if they have a decision making power in their mobility.
Moreover, the mobility and health care decision making’s vary in degree according the influence of economic decision making. For both surveys according of economic decision making the Normalized Beta value decreased due to control variable. (for 2005 survey N Beta value is 0.666, for 2016 survey is 0.911). Therefore, economic decision making influences to women’s health care and mobility empowerment decision making. Poverty is big burden on women in Ethiopia. They are denied access to, control over, financial resources. At the same time Ethiopian women should take a responsibility regarding household management (Mesfin 2004, 80-99).
Finally, there changes of women’s empowerment in Ethiopia between 2005 and 2016 survey periods. The differences of Normalized Beta value between 2005 and 2016 for mobility decision making is 1.16, for economic decision making is 0.786. According the statistical results, we may report that women empowerment in health care decision making among married women are changed positively. To the authors’ knowledge, many organizations such as UNWOMEN and United States Agency for International Development (USAID) have made a lot of efforts in improving the level of women’s empowerment in Ethiopia. United States Agency for International Development (USAID) focused on enhancing women’s social, economic, and political status. Providing educational and economic opportunities, enhancing women’s role policy, promoting the health safety of girls and women are the main goal of this project.
Consequently, based on the results we see the Ethiopian women as the potential costumers from the holistic perspective. This study discusses the about the possibility of the new market in health care industry. Therefore social quality management is critical issue in this context. Health policy makers have to figure out the market from the downstream stage. Furthermore policy makers and project organizations need to pay attention on the decision making issues of women in household level. Since, mobility and economic, health care decision makings are most likely made in family for married women, especially in some societies. Through the study we could see the changings the women’s empowerment in Ethiopia. In future if the women’s empowerment level of Ethiopian women will enhance continuously, the new market may open in health care industry.
The current study provided some implications regarding to women’s empowerment of Ethiopian women. However, we have to mention about some limitations of this study. Firstly, only 3 dimensions of women’s empowerment in household level were discussed in order to explore the health care decision making of women. Women’s empowerment is multidimensional concept with several levels and contexts. The health care decision making of women may be discussed by other factors, too. Future researchers may analyze the women’s empowerment in health care decision making with more dimensions. Secondly, the study focused on currently married women. Future studies may include all women and girls to understand women’s empowerment. In future through theses analyses it is important to figure out the potential costumers in the social quality level.





